








What conditions do we treat?
Nearly all of our patients come to us because of one of two types of problem: either they have one of a group of neurological conditions called 'movement disorders', or they are suffering from chronic severe pain of various kinds.
Movement disorders
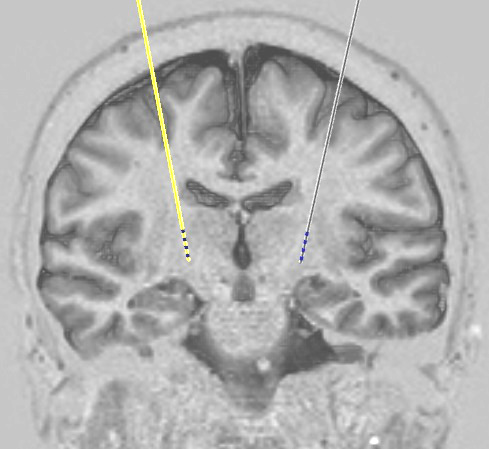
This group includes Parkinson's disease, dystonia, and tremor. These conditions can in some cases be treated by deep brain stimulation (DBS), a technique where wires are inserted into the brain to deliver small pulses of electricity to precisely targeted areas. Parkinson's disease is the commonest indication for DBS. There are several causes of tremor but the types we most often treat are Essential Tremor (ET), and midbrain tremor as seen in Multiple Sclerosis (MS).
Until quite recently it was often difficult to obtain NHS funding for DBS for movement disorders, but this is now routinely approved and is no longer a barrier to treatment in appropriate patients.
Patients do need to be selected carefully however, and DBS will not be the right answer for everyone. There are recognised criteria for DBS treatment that are available to help gauge whether a patient is a good candidate for surgery. When these are followed, treatment is usually successful, but unfortunately it does not work in every case.
More information can be found on our movement disorders page.
Pain
The best way to treat pain is to deal with its cause if possible. For example if a patient has pain in the legs due to a "slipped disc" in the back which is pressing on a nerve, we usually recommend an operation to remove the disc and this is in most cases successful. In the same way, pain in the hip due to arthritis is best treated with a hip replacement.
Sometimes there is no such easily addressable cause for pain. This may be because part of the nervous system has been damaged somehow and is malfunctioning and generating pain signals. For example, after removal of a slipped disc some people continue to have pain despite the fact that there is no longer any pressure on the nerve. Pain that results from injury to the nervous system is called "neuropathic" pain, and it can sometimes be very difficult to treat.
We treat patients with a range of different types of chronic severe neuropathic pain that has not responded to standard methods including trials of all appropriate medications, and is severe enough to have a substantial impact on their quality of life. The other group of painful conditions that we treat with neuromodulation are headache syndromes including migraine and cluster headache. More information about the pain conditions we treat and who might benefit from them can be found on our pain page.
Copyright OFN Wednesday, 11 February, 2015.
